Cataract surgery is performed to remove the eye's natural lens when it becomes cloudy due to cataracts, which can cause blurry vision, glare, and difficulty seeing at night. The cloudy lens is replaced with an artificial lens called an intraocular lens (IOL).
Phacoemulsification is a modern cataract surgery technique that involves breaking up the cataractous lens with ultrasonic waves and removing it through a small incision.
Pros:
Cons:

Phacoemulsification is a widely used and effective cataract surgery technique. Its small incision and quick recovery time make it a popular choice. However, it requires advanced surgical skills and may have potential complications. Discussing options with an eye doctor can help determine if phacoemulsification is the best choice for individual needs. With proper care and expertise, phacoemulsification can restore clear vision and improve quality of life.
Small Incision Cataract Surgery (SICS) is a surgical technique for cataract removal that involves a small incision and manual extraction of the cataractous lens.
Pros:
Cons:
SICS is a valuable technique for cataract removal, offering a cost-effective and efficient solution. While it may have some limitations, SICS provides excellent outcomes and is particularly useful in resource-limited settings. Discussing options with an eye doctor can help determine if SICS is the best choice for individual needs. With proper care and expertise, SICS can restore clear vision and improve quality of life.
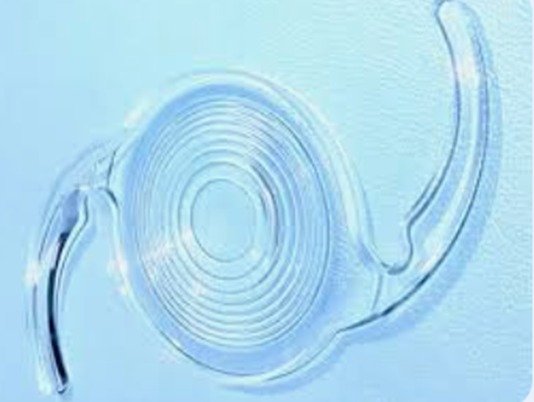
Intraocular lenses are artificial lenses implanted in the eye to replace the natural lens after cataract surgery. They restore vision by focusing light on the retina.

Foldable IOLs: Routinely used foldable IOLs are made of soft materials like acrylic. They are inserted through small incisions, reducing trauma and promoting faster healing. Examples include:
Rigid IOLs: Rigid IOLs, made of polymethylmethacrylate (PMMA), require larger incisions. Although less common today, they are still used in certain situations.
Specialized IOLs: Scleral Fixated IOLs: Used in cases of posterior capsule rupture or zonular weakness. These IOLs are sutured to the sclera for stability. Anterior Chamber IOLs: Used when posterior chamber placement is not feasible. These IOLs are placed in the anterior chamber angle. Iris clip lenses are also used in situations where the integrity of the capsule is in question.
These IOLs provide alternatives for complex cases, ensuring optimal visual outcomes for patients with unique needs.
Premium IOLs are advanced lens implants used in cataract surgery to improve vision at multiple distances. They're designed for patients seeking reduced dependence on glasses.
Types:
Pros:
Cons:
Considerations:
Discussing options with an eye doctor can help determine the best premium IOL for individual needs and preferences. By understanding the benefits and limitations, patients can make informed decisions about their vision correction.
If the cataract(s) are felt to be visually significant, surgical intervention is the only option. The timing of surgery is critical for visual development. Most investigators recommend surgery within the first two months of life. There has been evidence to suggest that before one month of age, the risk of aphakic glaucoma is increased. In cases of bilateral cataracts, it may be advantageous to perform surgery on both eyes in the same intervention to allow for simultaneous initiation of visual rehabilitation as well as reducing exposure to general anesthesia. In this setting, treating each eye as a separate sterile procedure may reduce infection risk.

Removal of the lens can be approached through the limbus or the pars plana. The limbal approach has the advantage of maintaining the posterior capsule to facilitate posterior chamber intraocular lens (IOL) implantation if desired.
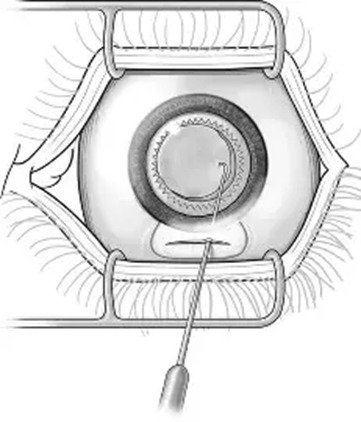
Several options exist to open the anterior capsule in pediatric cataracts. The ideal anterior capsulectomy technique is one that results in low incidence of radial tears and is easily performed. In cases of dense cataract, dye can be used to stain the anterior capsule, making this step easier and safer. A manual continuous curvilinear capsulorhexis (CCC), which is the preferred method in adult eyes, can be difficult in pediatric cases due to the elasticity of the pediatric capsule. However, when it can be controlled and completed, it creates an edge, which has a low incidence of radial tears. A 23 G vitreous end gripping forceps using push pull technique is very effective.
A mechanized circular anterior capsulectomy, known as vitrectorhexis has been proven to be a very good, safe alternative if the CCC is not possible. The vitrector tip is placed through a stab incision at the limbus and irrigation is provided though a sleeve around the vitrector or though a separate limbal incision. The vitrector port is oriented posteriorly, and held in the center of the capsule to create an initial opening. The opening is enlarged in a circular fashion, holding the cutter just anterior to the capsule to aspirate the capsule up into the cutter. A smooth, round capsulectomy that is also resistant to radial tears can be produced.
Pediatric cataracts are soft and therefore phacoemusification is generally not needed. The lens cortex and nucleus can be removed with an irrigation-aspiration or vitrector hand piece.
To reduce the risk of posterior capsule opacification most surgeons perform a posterior capsulorhexis at the time of surgery. The lens capsule can be filled with viscoelastic and a posterior continuous capsulorhexis made slightly smaller than the anterior one. If an IOL is to be implanted, it can be placed in the capsular bag at this time and some advocate the technique of optic capture where the optic is pressed through the posterior capsulorhexis and the haptics remain in the bag.
It is controversial whether an anterior vitrectomy should be performed at the primary surgery. It can be performed either through the limbal incisions, after making the posterior capsulotomy with the vitrector hand piece, or through the pars plana. The anterior vitreous is removed and the lens epithelial cells therefore cannot grow in the vitreous face.
IOL implantation in children is felt to be safe and acceptable in children as young as one year. In those younger than one year, the decision is more controversial and research is ongoing. The Infant Aphakia Study is investigating this and early results show good visual outcome.
The refractive goal of surgery is also controversial. Most surgeons will chose to make the child hyperopic but there is currently no agreed upon standard. These children will need bifocal glasses for the rest of their lives.
A pars plana approach can be used when no IOL implantation is intended. An attempt is made to remove the whole cataract and the adjacent vitreous with a vitreous cutter.
Care should be taken to remove the viscoelastic entirely to prevent elevated intraocular pressure following surgery and the anterior chamber should be checked carefully for vitreous. The sclera in children is soft and elastic and it is difficult to achieve a self-sealing incision, thus the incision should be closed using 10-0 nylon or Vicryl suture.
Managing Director
M.D.(AIIMS) D.N.B., F.RCS (Edinburgh & Glasgow)
stethoscope_arrow Cataract & IOL Services, LASIK & Refractive Surgery, Cornea Services, General Ophthalmology
event_available OP Days:
Monday,Tuesday,Thursday
DOMS, DNB, FICO
stethoscope_arrow Cataract & IOL Services, Paediatric Ophthalmology & Squint Services, General Ophthalmology
event_available OP Days:
Monday,Wednesday,Friday,Saturday

Medical Superintendent
MS, DNB, DO, FICO(UK), MRCS(Edin)
stethoscope_arrow Cataract & IOL Services, Uvea Services, General Ophthalmology
event_available OP Days:
Tuesday,Wednesday,Thursday,Saturday

MS, FICO
stethoscope_arrow Cataract & IOL Services, Glaucoma, General Ophthalmology
event_available OP Days:
Monday,Tuesday,Thursday,Saturday

D.O., D.N.B., MS, FRCS
stethoscope_arrow Vitreo Retina, Cataract & IOL Services, General Ophthalmology
event_available OP Days:
Thursday,Saturday

D.O., D.N.B., FICO,MRCS
stethoscope_arrow General Ophthalmology, Cataract & IOL Services, Community Ophthalmology
event_available OP Days:
Monday,Tuesday,Wednesday,Thursday,Friday,Saturday